
Cold-Reactive Autoantibodies - Confirmation:
The DAT will typically be positive for C3 only; this is because cold agglutinins are usually IgM, which both fix complement efficiently at colder temperatures and spontaneously elute from the RBC surface when the sample is warmed to 37ºC during the incubation phase of the antiglobulin test. Most commercial DAT kits can detect IgG class antibodies, with IgM antibodies inferred by the presence of isolated C3 deposition.
A typical cold-reactive autoantibody will have the following attributes:
- Agglutination is detectable with immediate spin only.
- Reaction strength increases with decreasing temperature.
- Reaction is equally strong with panel cells and patient cells.
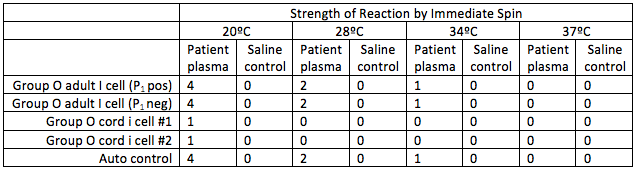
In the above example, the antibody specificity appears to be against the I antigen, which is the most common cause of cold agglutinin disease and typically occurs following Mycoplasma pneumoniae infections. Autoantibodies with anti-i specificity by contrast are more associated with EBV infections and lymphoproliferative disease, while even rarer anti-Pr antibodies have been reported following infections with varicella or Rubella viruses.
Anti-P1 cold agglutinins, which are usually benign, should not be confused with anti-P biphasic hemolysins, which are the cause of paroxysmal cold hemoglobinuria, a condition usually encountered in children following an infection. While these antibodies bind at cold temperatures, they are IgG class and thus not directly agglutinating and can only activate complement when warmed to 37ºC. Detection of biphasic hemolysins therefore requires Donath-Landsteiner testing, as described in Module 1.
Next page: Investigation